Drifts!!!
French neurologist Jean Alexandre Barré (1880–1967)

2) The four types of drift
3) Pronator drift (Barre’s sign)
progress from distal to proximal
1st downward arm drift
2nd forearm pronation
3rd flexion of the wrist and elbow

4) Pronator drift – assessment
5) Response

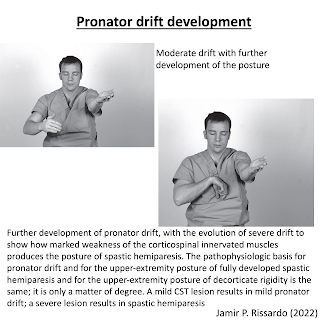
6) Pronator drift development
7) Clinical significance
a. can detect subtle upper motor neuron lesion which goes unrecognized by routine motor examination
b. included in initial examination of stroke
c. if only one motor test could be done in a patient – the best single test would be to examine the drift
8) Mechanism
Why pronator drift occurs when eyes are closed?
Why pronator overcomes supinator in pyramidal lesion?

9) Pronator drift
10) Pronator drift
11) Pronator drift
12) Drifts
13) Cerebellar drift
“drifts mainly outward, either at same level, rising, sinking”
- accentuated by raise&lower arms or tapping wrists
- ipsilateral
14) Parietal drift
i) can be ‘out, up or rarely downward’
ii) parieto-occipital lesion out&upward
iii) parieto-temporal lesion up but NOT outward
- contralateral lesion
- Brodmann area relation

15) Parietal drift
16) Functional drift

17) Leg drift