Guillain-Barre syndrome

Georges Charles Guillain (1876-1971)
Jean Alexandre Barré (1880-1967)
André Strohl (1887-1977)
“diagnosed two soldiers with a condition similar to Landry paralysis”
2) Definition
“acute immune-mediated polyneuropathies”
3) Epidemiology
C. jejuni – MC infectious etiology
M. pneumoniae – MC in children
*Others: HEV, CMV, EBV
Prodrome
- Respiratory MC in Europe and North America
- Diarrheal MC in Asia
4)Time
“should not progress more than 4 weeks”

*consider acute on CIDP, if > 3 relapses or more than 8 weeks
5) Diagnostic criteria
Req
- progressive weakness
- hyporeflexia (appears within 1 wk)
Sup
- prog over 4 weeks
- symmetry
- mild sensory
- CN involvement
- autonomic dysfunction
- pain
- elevated CSF protein
- EMG features
6) GBS classification
- based on clinical and neurophysiological features

7) GBS variants
- axonal
- localized
- Miller Fisher syndrome
8) Axonals
- AMAN & AMSAN
- AMAN 2 patterns of recovery: quick (conduction block resolution) or slow (extensive axonal degeneration)
9) Miller Fisher syndrome
- triad ophthalmoplegia, ataxia, and areflexia
- Bickerstaff brainstem encephalitis: MFS + impaired consciousness and paradoxical hyperreflexia
10) Pathogenesis
- molecular mimicry
- neural target
- AIDP vs AMAN
> AIDP: multifocal perivascular and endoneurial T-cell infiltration, prox and distal (weak BBB)
> AMAN: anti-ganglioside binding, complement activation & MAC
11) LP & EMG & MRI
- LP before IVIG because alters WBC & protein count
- EMG should be later repeated
- Spinal MRI w/ thickening and enhancement of intrathecal spinal nerve roots
12) Ganglioside target

13) Treatment

Prompt Neuro ICU
- dysautonomia, bulbar dysfunction, severe or rapidly worsening weakness, and evolving respiratory distress
- GBS scale > 4
Dysautonomia
- profound dysautonomia at intubation
IVIg versus PLEX
- repeating IVIg or PLEX for absence of clinical response after initial treatment for GBS provides no additional benefit
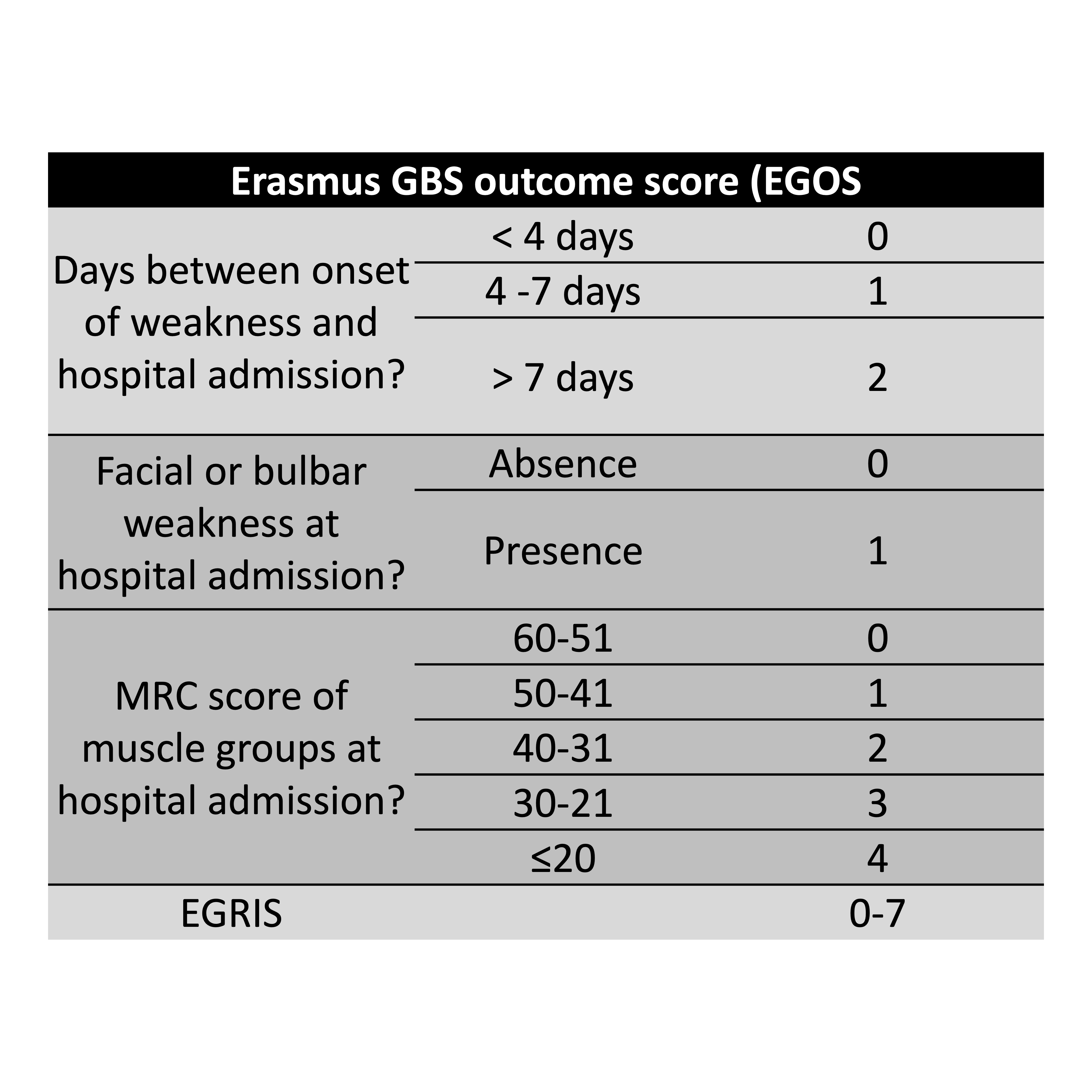
14) Erasmus GBS outcome score (EGOS)