Six Syndromes of the Sixth Cranial Nerve
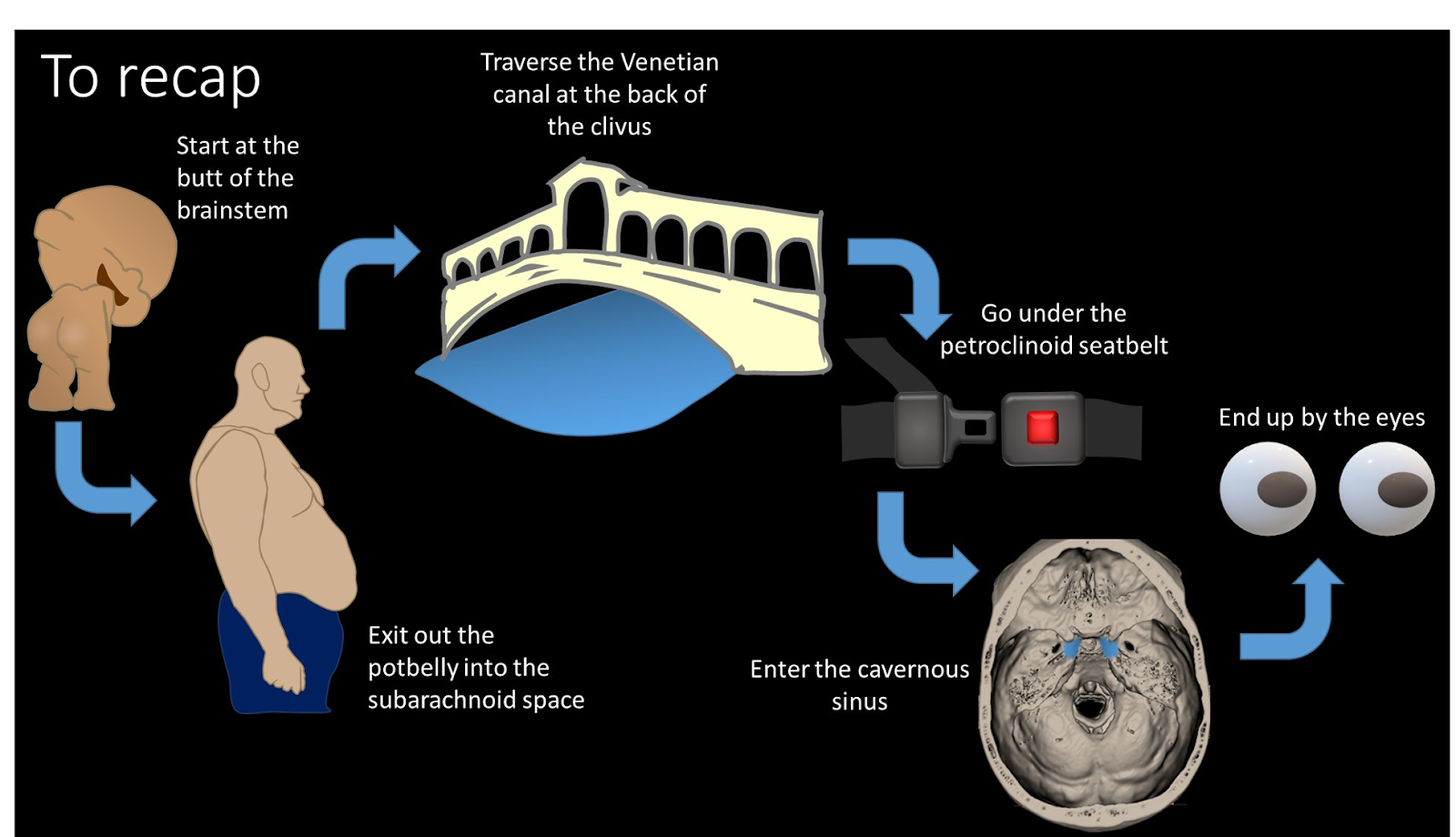
2) To understand the six syndromes, you have to know the anatomy of the 6th nerve. It starts in the brainstem, at the facial colliculus—what looks like the butt of the brainstem. It then travels anteriorly through the brainstem to exit out the ventral surface of the pons.3) It exits the brainstem at the inferior aspect of the pons—under what looks like pot belly of the pons and then travels anteriorly in the subarachnoid space towards the clivus
4) It then enters Dorello canal, a channel at the lateral aspect of the posterior clivus, right by the petrous bone. This canal travels superiorly—taking the nerve up towards the orbit, where it will eventually end up
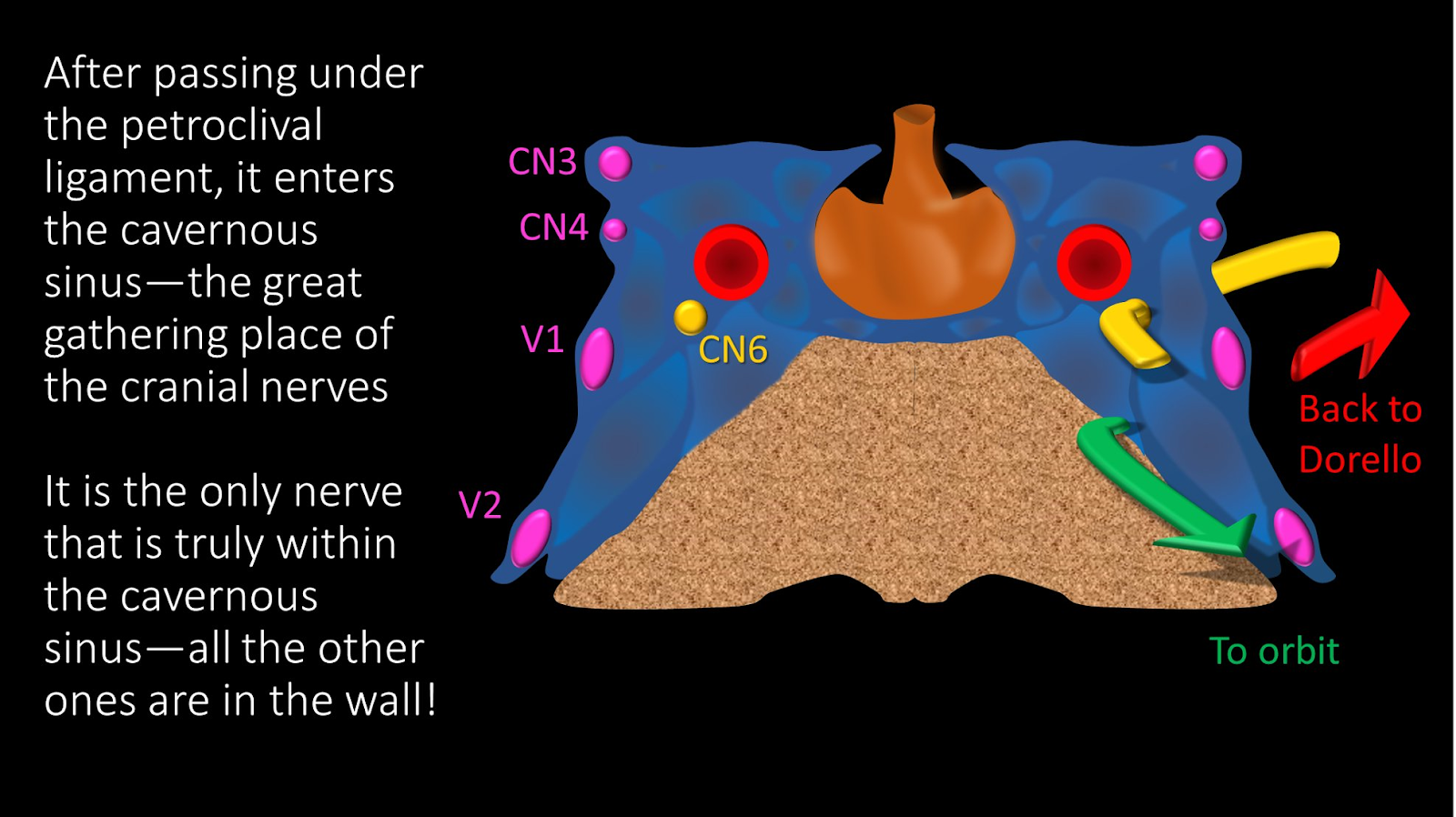
5) The exit of Dorello canal is marked by the petroclinoid ligament. Which, as its name implies, runs between the petrous ridge and clinoid. The 6th nerve runs under this ligament, which holds it down against the medial petrous ridge like a seatbelt
6) It then enters the cavernous sinus, where cranial nerves 3, 4, and 5, as well as the ICA and sympathetics also run. It is located more medially than the other nerves—in fact, it is the only nerve to run in the cavernous sinus itself, rather than in the wall
7) It exits the cavernous sinus to enter the orbit through the superior orbital fissure. Here, it is joined in the SOF by CN 3 and 5, with CN 2 in close proximity. As soon as it enters the orbit, it makes an immediate turn laterally and innervates the lateral rectus muscle8) Here is a recap of the course of the 6th nerve. Remember it—because where the pathology is along the course of the nerve will determine which syndrome we will see!
9) At each point of the course, injury to the nerve will cause a different syndrome—giving us the 6 syndromes of the 6th cranial nerve!
10) The syndrome we get depends on the location of the lesion. Here are the syndromes laid out against the region of the cranial nerve course they are associated with
11) In the brainstem, there are many important structures in close proximity to 6th nerve nucleus and its course through the brainstem before it exits. Notably, the pyramidal tracts containing your motor fibers are in direct proximity with the intraaxial 6th nerve.
12) Compressive, ischemic or inflammatory lesions may affect CN6 here, but likely other CNs & pyramids will be affected. There are specific syndromes, but key point--if there are other deficits, especially MOTOR, a deficit unique to brainstem lesions—it’s time to call neurology!
13) As it travels through the subarachnoid space & into Dorello canal, it is susceptible to changes in intracranial pressure. B/c it is tethered in Dorello canal, if the brainstem moves with changes in pressure, it is stretched. This can uniquely give bilateral isolated palsies
14) As it exits Dorello & travels under the petroclinoid ligament, petrous apex infections from complicated otitis media, can affect it. This region rarely gives an isolated palsy b/c other nerves are here. So if it's a complex palsy with hearing symptoms—think of this region!15) After it enters the cavernous sinus, things get complicated. B/c of all the nerves in close proximity, isolated palsies are rare here. Cavernous sinus syndrome is deficits of two or more of these structures. Both the deficits & differential diagnosis are extensive!16) It then enters the orbit—and immediately takes a lateral turn after the SOF to innervate the superior rectus. So not much of the length of the nerve is separated from the other nerves, & lesions here will cause a SOF syndrome or orbital apex syndrome, not an isolated palsy17) Last syndrome is, if there is no other identifiable cause—the transverse myelitis of CN6! (likely microvascular/post-inflammatory). But you must rule out the other 5 syndromes first!
Reference: Lea Alhilali, https://twitter.com/teachplaygrub/status/1525117898733170688













 17) Last syndrome is, if there is no other identifiable cause—the transverse myelitis of CN6! (likely microvascular/post-inflammatory). But you must rule out the other 5 syndromes first!
17) Last syndrome is, if there is no other identifiable cause—the transverse myelitis of CN6! (likely microvascular/post-inflammatory). But you must rule out the other 5 syndromes first!
 Reference: Lea Alhilali, https://twitter.com/teachplaygrub/status/1525117898733170688
Reference: Lea Alhilali, https://twitter.com/teachplaygrub/status/1525117898733170688