Article type: Case Report and Literature Review
Article title: Cortical (Spastic) Isolated Unilateral Foot Drop: The Foot Knob Area
Journal: The Neurohospitalist
Year: 2024
Authors: Jamir Pitton Rissardo, Ana Letícia Fornari Caprara
E-mail: jamirrissardo@gmail.com
ABSTRACT
Foot drop is a condition characterized by impairment of the ability to dorsiflex the foot at the ankle joint. We aim to review the literature and report a case of isolated unilateral foot drop of central causes. A 59-year-old male previously healthy presenting with a right foot drop was admitted. Severe weakness of ankle dorsiflexion with intact plantar flexion was observed. Deep tendon reflexes were normal, no clonus was appreciated, and a plantar response resulted in flexion of all toes. Neuroimaging showed a lesion in the high left frontal lobe, centered along the medial aspect of the precentral gyrus. Levetiracetam and dexamethasone were started, and after four days, the patient reported a slight improvement in his ability to dorsiflex his ankle. Abdominal imaging showed a large right renal mass with invasion of the renal pelvis fat, suggestive of renal cell carcinoma, and cytology diagnosed clear cell renal cell carcinoma. There are 25 articles containing 33 individuals with unilateral foot drop secondary to non-traumatic central causes in the literature. The mean and median age were 50.26 (SD = 20.57) and 55.5 years old (12 - 79 years). Most of the patients were males, which accounted for 55.88% (19/34). The side of the foot drop was right at 58.82% (20/34).
Keywords: cortical foot; deep fibular; deep peroneal; foot drop; foot knob area; meningioma; parasagittal; spastic foot.
Full text available at:
DOI
Citation
Rissardo JP, Fornari Caprara AL. Cortical (Spastic) Isolated Unilateral Foot Drop: The Foot Knob Area. Neurohospitalist 2024;15:136–150.
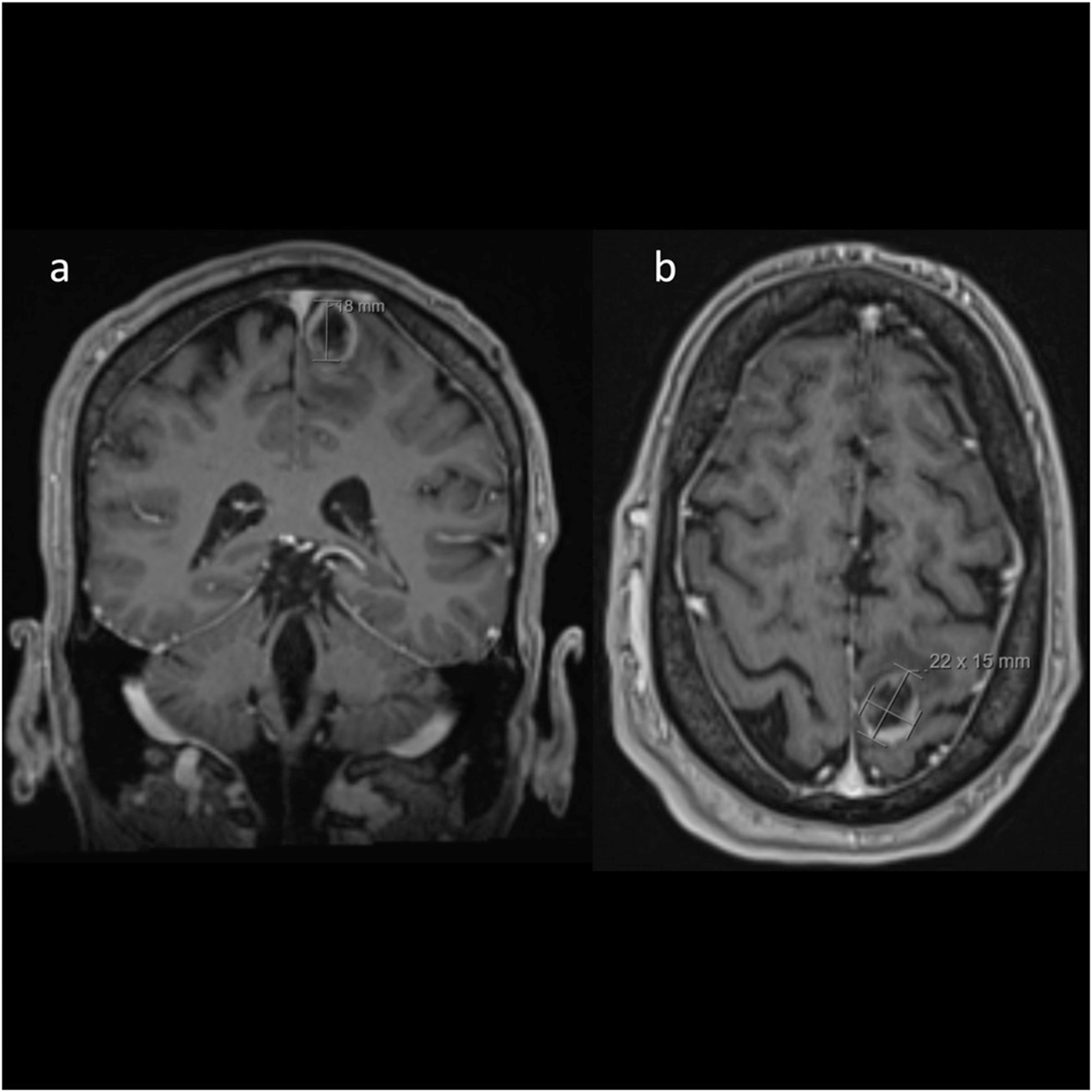
Figure 1. Dimensions of the lesion in the high left frontal lobe, centered along the medial aspect of the precentral gyrus, measuring 2.2 x 1.5 x 1.8 cm.

Figure 2. Axial views. (A) Apparent diffusion coefficient; (B) Trace diffusion-weighted; (C) Fractional anisotropy; (D) Fluid attenuated inversion recovery; (E) T2-weighted gradient echo; (F) T1 Turbo spin echo (TSE/FS); (G) T2-weighted fat-suppressed; (H) T1-weighted.

Figure 3. Sagittal and coronal views. (A) Sagittal T1; (B) Coronal T2; (C) Coronal T1 Turbo spin echo (TSE/FS); (D) 3D T1 magnetizationprepared rapid gradient echo (MPRAGE).

Table 1. Case Reports of Cortical (Spastic) Isolated Unilateral foot Drop Published in the Literature.

Table 2. Causes of foot Drop Separated by Neurolocalization.